Survey Instructions
19 CSR 30-105.010 (11) Health care personnel or personnel shall mean any individual licensed, accredited, or certified by the state of Missouri to perform specified health services consistent with state law.
19 CSR 30-105.010 (13) Independent contractor shall mean a self-employed worker licensed, accredited, or certified by the state of Missouri to perform specified health services consistent with state law, who is contracted, referred, or provisioned for engagement by a supplemental health care services agency to fulfill specified health services in a health care facility.
19 CSR 30-105.010 (19) Specified health service shall mean services provided by any individual health care personnel or independent contractor in a health care facility.
Health care personnel defined in 198.640(4) include:
- Certified Medication Technician (CMT)
- Certified Nursing Aide (CNA)
- Dietitian
- Emergency Medical Tech (EMT) (ER only)
- Hearing Instrument Specialist
- Level One Medication Aide (LIMA)
- Licensed Practical Nurse (LPN)
- Occupational Therapist
- Occupational Therapist Assistant
- Paramedic (ER only)
- Perfusionist
- Pharmacy Technician
- Physical Therapy Assistant
- Registered Nurse (RN)
- Speech Language Aide
Health care personnel not listed above are not included in this survey and are not required to be reported to MO DHSS. If you have a health care personnel not listed above that you believe falls within 198.640(4) please contact the SHCSA team.
Health care facilities to be reported are Hospital’s or Long-term Care Facility’s ONLY that participate in Medicare or Medicaid.
SHCSA Quarterly Survey Instructions
*Instructions include 1st quarter data examples and will not be updated within the instructions each quarter*
*If your agency does not pay specific personnel, you would not include them on the survey.
*If RN A and RN B work at the same facility, and their average pay is identical, only list the RN and pay once.
*Quarterly reporting is required even if an agency did not contract with any health care facility (Hospital or Long-term Care Facility) that participates in Medicare or Medicaid, and/or if your agency did not have personnel working in Missouri during the reporting quarter.
Once in the survey, select your agency name:

*If you select the incorrect agency name, delete/backspace the name and reselect.
*If you were issued an approved registration and do not see your agency name in the drop down please contact SHCSA@health.mo.gov or 573- 526-5335
Next, verify your registration number and agency address:
The quarter the department is collecting data on will automatically be selected:

- The quarterly report containing data from January 1 through March 31 opens April 1 and shall be submitted no later than April 30;
- The quarterly report containing data from April 1 through June 30 opens July 1 and shall be submitted no later than July 31;
- The quarterly report containing data from July 1 through September 30 opens October 1 and shall be submitted no later than October 31;
- The quarterly report containing data from October 1 through December 31 opens January 1 and shall be submitted no later than January 31.
Next, select if your agency contracts with any health care facility (Hospital or Long-term Care Facility) that participates in Medicare or Medicaid, and if your agency had personnel working in Missouri during the reporting quarter:
*You may verify if a hospital is Medicare/Medicaid certified here if a CMS Provider # is listed.
*You may verify if a LTC facility is Medicare/Medicaid certified here if Medicare/Medicaid is listed under the Certification column.
Fill in the submitter information. Be sure to include a direct phone number and extension if applicable to get in immediate contact with the submitter. *The email listed will be sent survey reminders in the future:
*If you selected no on either question: Does your agency contract with any health care facility that participates in Medicare or Medicaid? OR Did your agency have personnel or independent contractors working in Missouri between January 1, 2024 and March 31, 2024? Click submit and you are finished.
*If you selected yes on both of the first two questions above, please click on the Open Quarterly Survey Template.
*The Quarterly Survey Template Excel file is updated each quarter, please do not reuse a worksheet uploaded from a prior quarter OR create your own worksheet. It will not be accepted!!
A message may pop up asking to leave the site? Click Leave and the Excel document will download in your browser (this may look different depending on what browsing source you use):
Click on and open the Quarterly Survey Template:
Once the Excel template opens on your desktop, click Enable Editing at the top of the Excel:

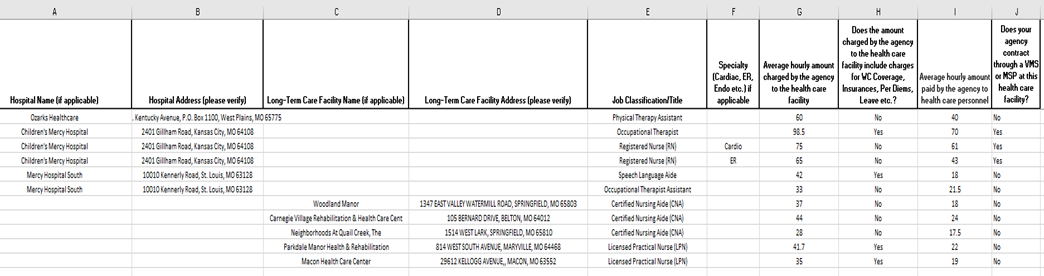
Enter applicable data in each row for each job classification/title and each health care facility personnel works at.
Hospital and Long-term Care Facility names are included under the applicable column, please select and verify the facility address.

Select from the drop down the Job Classification/Title:
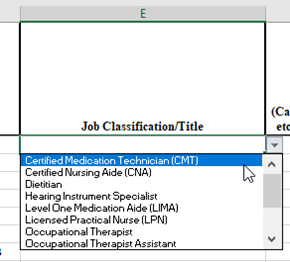
*Do not fill in facility information, please make selections from the options available. The address should automatically populate after a facility name has been selected. If you do not see a hospital or LTC listed that your agency contracts with, please notify the SHCSA team.
Here is a brief example of the entire template filled out:
Once complete, save the Excel file to your computer and upload the file to the Drop file here or select file box. After the file shows it has been uploaded, click submit and you are finished:
*REMINDER: The list of Hospital and Long-term Care Facility names are updated each quarter; a new excel sheet should be downloaded each quarter to reflect changes.
* If a survey was submitted and was incorrect please call 573-526-5335 before resubmitting another survey.
Any questions should be directed to SHCSA@health.mo.gov or 573-526-5335