Primary Congenital Hypothyroidism
Brief Description
Congenital hypothyroidism (CH) are disorders of the thyroid-hypothalamus-pituitary axis resulting in inadequate production of thyroid hormones which is necessary for normal metabolism, growth, and brain development. Hypothyroidism is a family of disorders, including endemic cretinism, thyroid agenesis or ectopia, genetic disorders of thyroid hormonogenesis, or hypopituitarism.
Laboratory Unit
Methodology
Immunofluoresence Assay
Analyte measured: Thyrotropin (TSH - Thyroid Stimulating Hormone)
Specimen Collection
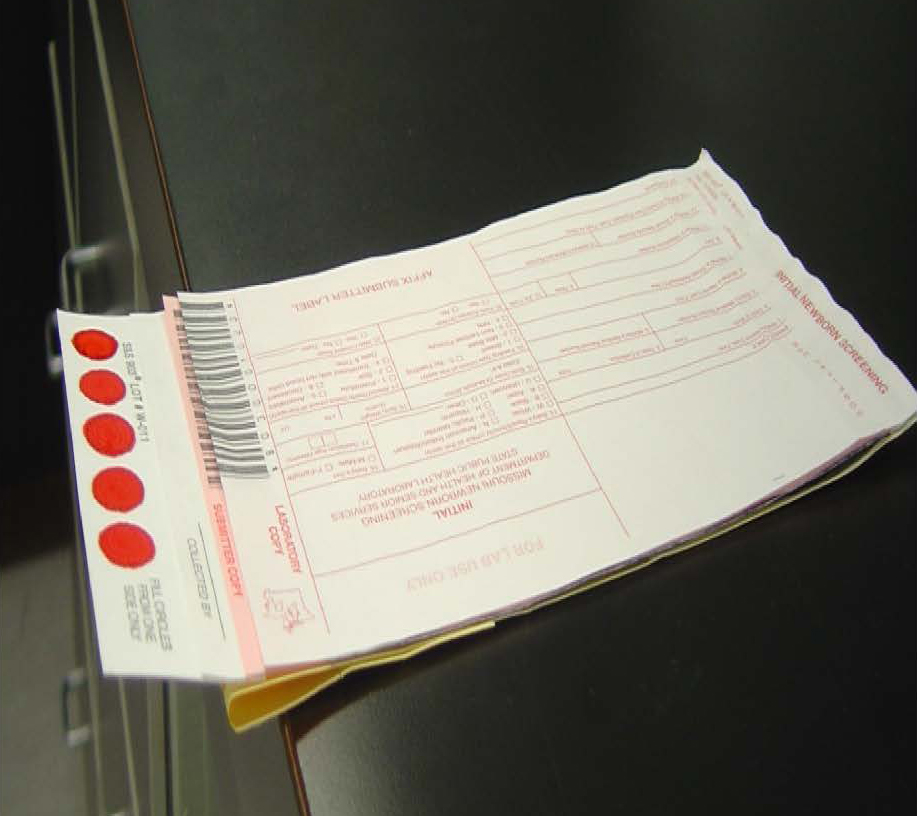
Missouri newborn screening samples must only be collected on the Food and Drug Administration (FDA) approved blood collection forms that must be pre-purchased from the MSPHL. The optimum collection time is between 24 and 48 hours-of-age. The instructions for collecting the samples are listed on the back of the collection form. All 5 circles on the filter paper need to be filled with blood from one side and then air dried for at least 3 hours in a horizontal position without allowing the blood to touch any surface during drying, including other parts of the card. (Example on the right)
Storage/Transport
Store the dried blood samples at room temperature in the envelopes provided by the MSPHL and transport within 24 hours of collection.
Acceptable Specimen Type(s)
Initial Screen (the red form) or Repeat Screen (the green form)
Test Request Form(s)
Included in kit
Possible Results
Normal - The final newborn screening reports are mailed to the submitter and physician of record.
Borderline Risk - Repeat the newborn screen or do serum testing. The final newborn screening reports are mailed to the submitter and physician of record.
High Risk - Diagnostic thyroid serum testing and consultation with an endocrinologist is needed. Final results are phoned and faxed to physician/health care provider and appropriate follow up center. Follow up centers are contracted by the Department of Health and Senior Services (DHSS) for follow up tracking, testing, diagnosis, and counseling.
No Result - All specimens collected before 24 hours of age are invalid and are given a "No Result". A repeat newborn screen is requested.
Interpretation of Newborn Screening Results for TSH
Interfering Substances
Premature, low birth weight, sick NICU (Neonatal Intensive Care Unit) infants have been documented to develop a late onset form of CH.
Specimen collection prior to 24 hours of age, prematurity, and illness can all affect the newborn screening results.
False positives may occur due to early specimen collection. In the first day of life, TSH levels may be transiently elevated. TSH increases dramatically shortly after birth and gradually returns to adult normal levels in about 72 hours. False positive results occur due to the specimen being collected at the height of the TSH spike, usually within the first 24 hours of life. For this reason “No Result” is reported on those specimens collected before 24 hours of age. TSH levels should begin to return to normal levels within 24 – 48 hours following birth. Other factors that can affect thyroid hormone levels and result in abnormal screening results are prematurity, maternal medication, such as anti-thyroid drugs, or topical iodine treatment.
The false-negative rate for CH on the first newborn screening specimen is higher than all of the other disorders screened. Therefore, even if the newborn screening results are normal, the physician must remain alert to clinical symptoms in older infants and/or a family history of thyroid disorders. Perform diagnostic thyroid serum testing if any doubt exists.
Although newborn screening can detect “primary” hypothyroidism with a high degree of accuracy, delayed hypothyroidism and other forms of hypothyroidism may develop in the weeks after birth.
Result Reported
1 to 3 working days after receipt of specimen.
Fees
$130 charge - for full panel of screening disorders.
CPT Codes
84443
LOINC/SNOMED Codes
N/A
Additional Information
Prevalence of Disorder: 1 in 1,600 in Missouri
Types Detected: There are several types of primary CH, the most common form resulting from abnormal fetal development of the thyroid gland. The thyroid gland may be absent, mislocated (ectopic) or malformed. Transient hypothyroidism may occur in some infants as a result of maternal exposure to excess iodine, anti-thyroid medication (propylthiouracil or PTU), or exposure of the infant to maternal anti-thyroid antibodies. The use of iodine-based skin disinfectants on neonates, especially premature neonates, can inhibit thyroxine production resulting in transient hypothyroidism. Although newborn screening can detect "primary" hypothyroidism with a high degree of accuracy, delayed hypothyroidism and other forms of hypothyroidism may develop in the weeks after birth.
For more information on this Disorder, visit the DHSS Newborn Screening website.