Congenital Adrenal Hyperplasia (CAH)
Brief Description
A family of diseases whose common feature is an enzymatic defect in the steroidogenic pathway leading to the biosynthesis of cortisol. The 21-hydroxylase deficiency accounts for 90 to 95 percent of CAH cases, resulting in ambiguous genitalia in females and salt-losing crisis in either males or females. Early detection and treatment is essential to prevent death in infants with salt-losing CAH.
Laboratory Unit
Methodology
Immunofluoresence Assay
Analyte measured: 17 α-hydroxyprogesterone (measure in ng/ml)
Specimen Collection
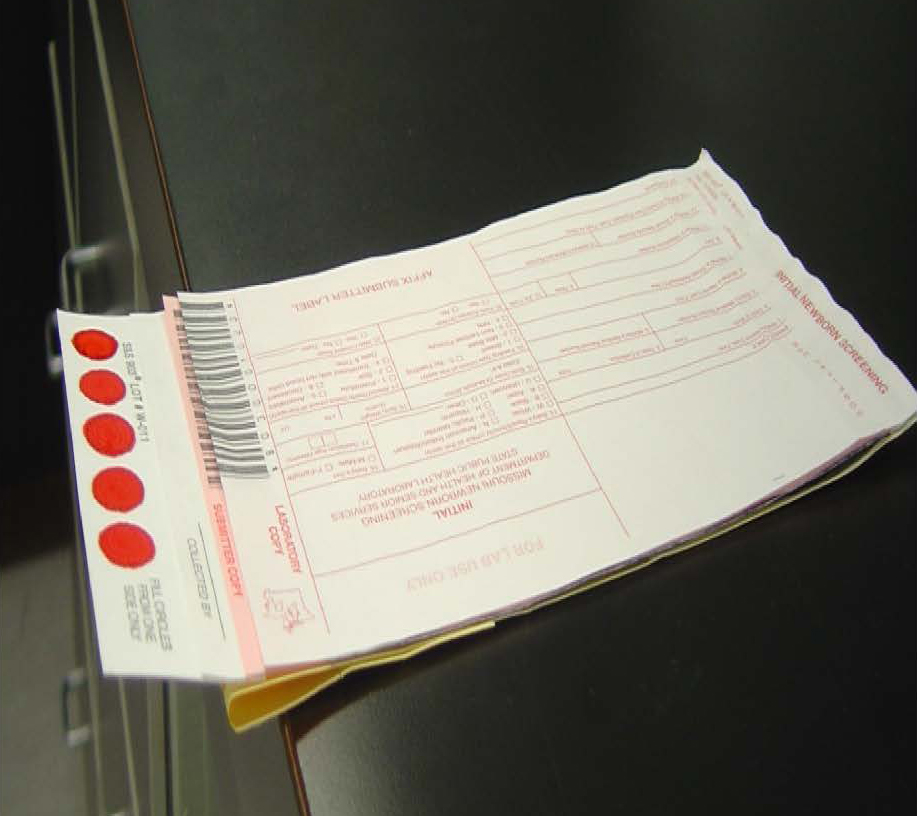
Missouri newborn screening samples must only be collected on the Food and Drug Administration (FDA) approved blood collection forms that must be pre-purchased from the MSPHL. The optimum collection time is between 24 and 48 hours-of-age. The instructions for collecting the samples are listed on the back of the collection form. All 5 circles on the filter paper need to be filled with blood from one side and then air dried for at least 3 hours in a horizontal position without allowing the blood to touch any surface during drying, including other parts of the card. (Example on the right)
Storage/Transport
Store the dried blood samples at room temperature in the envelopes provided by the MSPHL and transport within 24 hours of collection.
Acceptable Specimen Type(s)
Initial Screen (the red form) or Repeat Screen (the green form)
Test Request Form(s)
Included in kit
Possible Results
Normal - The final newborn screening reports are mailed to the submitter and physician of record.
Borderline Risk - 17-OHP results in the Borderline risk range should be followed up promptly with a repeat newborn screen or with a serum 17-OHP. If clinical symptoms of salt-wasting CAH are present, consult with a pediatric endocrinologist and confirm with serum testing. The final newborn screening reports are mailed to the submitter and physician of record.
High Risk - 17-OHP results in the High Risk range should be considered a medical emergency until the patient has been evaluated to confirm or rule out the diagnosis of salt-wasting CAH. Final newborn screening results are phoned and faxed to physician/health care provider and appropriate follow up center. Follow up centers are contracted by the Department of Health and Senior Services for follow up tracking, testing, diagnosis, and counseling.
No Result - All specimens collected before 24 hours of age are invalid and are given a "No Result." A repeat newborn screen is requested.
Interfering Substances
Hormone (steroid) therapy administered to the mother during pregnancy, or to the infant immediately after birth, can interfere with CAH test results. Cross reactivity with other precursor hormones present in premature infants may also cause false positive results.
Premature or sick infants may have a false-positive screen due to increased stress on the body. Because the immature adrenal gland sustains increased plasma concentrations of most adrenal metabolites, including those measured to detect CAH, elevated levels of 17-OHP may be detected in premature infants. Additionally, the stress of illness commonly experienced by premature infants also stimulates adrenal steroid production.
Specimens collected prior to 24 hours of age may exhibit a false positive or false negative result. It is extremely important to perform a second screening on these infants as soon as possible to ensure that the infant whose 17-OHP level has not stabilized, and is continuing to rise, is not missed. A small percent of infants will be detected only on a second screen.
Blood collection with preservatives (EDTA) can result in false positive results.
CAH ranges apply to the newborn period. Interpretation of results from specimens collected after the newborn period should be performed in consultation with a pediatric endocrinologist.
Result Reported
1 to 3 working days after receipt of specimen
Fees
$130 charge - for full panel of screening disorders.
CPT Codes
83498
LOINC/SNOMED Codes
N/A
Additional Information
Prevalence of Disorder: 1:20,000 in Missouri
Types Detected: The screening test for CAH is meant to identify infants at risk and in need of diagnostic testing. A “normal” screening result does not rule out the possibility of a “non-salt wasting” form of CAH, a mild form of 21-hydroxylase deficiency CAH, or other forms of CAH.
The most frequent types of CAH are 21-hydroxylase deficiency (about 80% of all cases) and 11-β-hydroxylase efficiency (about 15% of all cases). Other types (lipoid adrenal hyperplasia or 20α-hydroxylase deficiency, and 3β-hydroxysteroid dehydrogenase deficiency) are very rare. 17-α-OH-progesterone, a precursor of cortisol, is increased in both 21- and 11-β-hydroxylase deficiency the two most frequent types of CAH, but not in the other types. Its determination is thus useful as a screening method for the two most frequent types of CAH, or about 95% of all cases. If CAH is diagnosed by the screening procedure, differentiation between 21- and 11 β-hydroxylase deficiency has to be carried out later on. Late onset non-classic CAH is not accurately detected by newborn screening.
Infants with CAH may not appear ill at birth, but may experience a salt-losing crisis within the first few weeks of life, which can lead to serious illness and death. Be alert for possible symptoms of salt-wasting CAH: poor feeding, lethargy, vomiting, dehydration, hypotension and ambiguous genitalia. Consult with a pediatric endocrinologist. Male infants with CAH are normal at birth. In severe cases, salt wasting becomes evident within 7-10 days. By 2-3 weeks, failure to thrive, unexplained vomiting, poor feeding, hypovolemia and shock develop. The same sequence of symptoms develops in untreated female infants with CAH, but virilization with sexual ambiguity at birth leads to an early diagnosis of CAH and adequate treatment in many patients. However, complete female virilization presents at birth with the clinical phenotype of a male infant. In this presentation, the diagnosis of CAH may be missed and the incorrect sex assigned. Approximately 75% of children with classic CAH have the salt-losing CAH.
The simple virilizing form of CAH is seen in approximately 25% of those with 21-hydroxylase deficiency. Simple Virilizing CAH have normal aldosterone secretion and present with excessive prenatal production of androgens in affected females resulting in masculinization of the reproductive tract to a point that the sex of the newborn is not clear ("ambiguous genitalia") or appears male-like. Affected males are usually normal at birth. The diagnosis in boys may not be evident until childhood. Late diagnosis is associated with markedly advanced skeletal maturation and accelerated linear growth initially, but early natural puberty and ultimately short stature.
Still milder forms of 21-hydroxylase deficiency are referred to as non-classical CAH and can cause androgen or masculinization and infertility in adolescent and adult women. The newborn screening test usually does not detect attenuated or late onset non-classical CAH patients.
Reference and Support Groups
Congenital Adrenal Hyperplasia Research, Education and Support Foundation (CARES) 11 Hardwell Road, Short Hills, NJ 07078 Phone: 1-866-227-3737
MAGIC Foundation for Children’s Growth 1327 North Harlem Avenue, Oak Park, IL Phone: 1-800-362-4423
National Adrenal Diseases Foundation (NADF) 505 Northern Blvd., Great Neck, NY 11021 Phone: 516-487-4992
The John Hopkins Children’s Center