Biotinidase Deficiency
Brief Description
An inherited metabolic autosomal recessive disorder of biotin (Vitamin B complex) recycling that leads to multiple carboxylase deficiencies. Carboxylases are important in the production of certain fats and carbohydrates, and for the breakdown of proteins. Individuals with biotinidase deficiency cannot recycle endogenous biotin and cannot release dietary protein-bound biotin.
Laboratory Unit
Methodology
Assay combines an enzyme reaction with a solid phase time-resolved immunofluorescence assay.
Analyte measured: Biotinidase
Specimen Collection
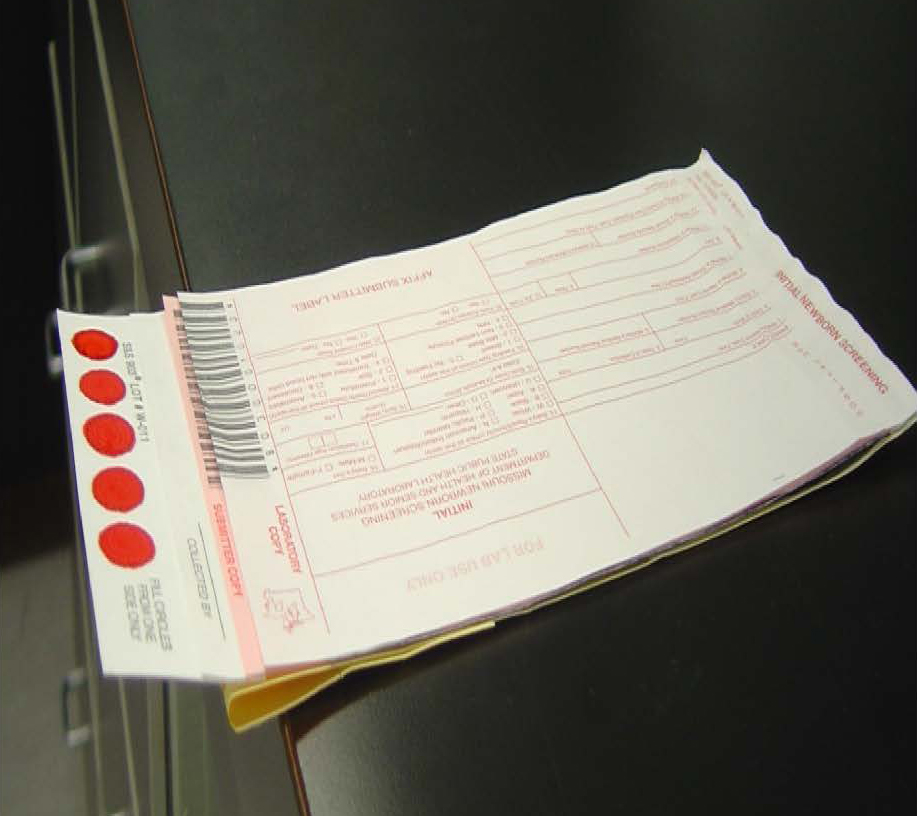
Missouri newborn screening samples must only be collected on the Food and Drug Administration (FDA) approved blood collection forms that must be pre-purchased from the MSPHL. The optimum collection time is between 24 and 48 hours-of-age. The instructions for collecting the samples are listed on the back of the collection form. All 5 circles on the filter paper need to be filled with blood from one side and then air dried for at least 3 hours in a horizontal position without allowing the blood to touch any surface during drying, including other parts of the card. (Example on the right)
Storage/Transport
Store the dried blood samples at room temperature in the envelopes provided by the MSPHL and transport within 24 hours of collection.
Acceptable Specimen Type(s)
Initial Screen (the red form) or Repeat Screen (the green form)
Test Request Form(s)
Included in kit
Possible Results
- Normal: The final newborn screening reports are mailed to the submitter and physician of record.
- Borderline Risk: Biotinidase is decreased. Repeat the newborn screen. The final newborn screening reports are mailed to the submitter and physician of record.
- High Risk:Biotinidase is decreased or absent. Final results are phoned and faxed to physician/health care provider and appropriate follow up center. Follow up centers are contracted by the Department of Health and Senior Services (DHSS) for follow up tracking, testing, diagnosis, and counseling. Final newborn screening report is mailed to the submitter and physician of record.
Interpretation of Newborn Screening Results
Interfering Substances
The Biotinidase screening results are unaffected even if the specimen is obtained before formula or milk feeds or collected before 24 hours of age, unless the infant has been transfused.
NICU Guidelines and Key for NBS
- Pre-transfusion: at any hour of age results are valid
- Post-transfusion: Greater than, equal to 30 days post transfusion results are valid
False negative Biotinidase Deficiency results may occur in infants if they:
- are being treated with antibiotics
- have been recently transfused
Infants who need a transfusion or antibiotics should be screened prior to instituting these therapies.
False positive results may be caused by:
- improper collection technique or improper handling of sample
- improper drying
- samples placed in plastic prior to drying
- delayed transit or exposure to heat and humidity
- impaired liver function
- prematurity
- infants with severe jaundice
Proper collection, drying techniques and reducing transit delays can help to reduce false positive results.
Result Reported
1 to 3 working days after receipt of specimen
Fees
$130 charge - for full panel of screening disorders.
CPT Codes
82261
LOINC/SNOMED Codes
N/A
Additional Information
Prevalence of Disorder: Profound and Partial Biotinidase Deficiency in Missouri is 1:5,500
Follow Up Testing and Treatment: Follow up testing usually includes a quantitative biotinidase serum assay and mutation testing that determines the genotype of the baby. Other tests may be ordered for diagnosis.
Decreased Biotinidase levels require prompt diagnostic testing to determine if the baby has biotinidase deficiency or is a carrier for the disease. It is highly recommended that the baby’s physician/health care provider contact one of the Newborn Screening Follow Up Centers (see below) for consultation, diagnosis, and treatment. Early detection for Biotinidase Deficiency is crucial.
Variant Forms of Biotinidase Deficiency: There are several genetic variants characterized by less severe reduction in the enzyme activity. Although most of these individuals are asymptomatic, all should be evaluated, as some will require management and monitoring.
For more information on this Disorder, visit the DHSS Newborn Screening website.