Fatty Acid Disorders
Brief Description
In these metabolic disorders enzymes necessary for the breakdown of fatty acids, which produces energy, are unavailable or have reduced activity. Affected newborns can develop symptoms and suffer metabolic crisis as early as 24 hours after birth. Newborns identified to be at risk for a fatty acid disorder are referred to a contracted medical center for diagnostic evaluation.
Laboratory Unit
Methodology
Tandem Mass Spectrometry (MSMS)
Specimen Collection
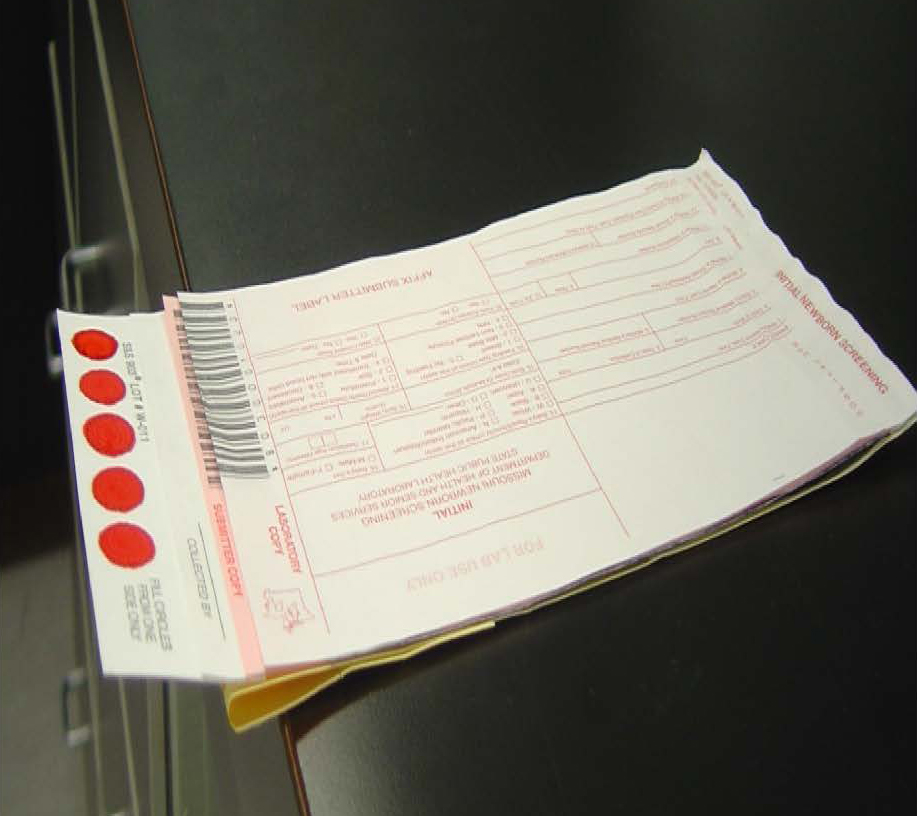
Missouri newborn screening samples must only be collected on the Food and Drug Administration (FDA) approved blood collection forms that must be pre-purchased from the MSPHL. The optimum collection time is between 24 and 48 hours-of-age. The instructions for collecting the samples are listed on the back of the collection form. All 5 circles on the filter paper need to be filled with blood from one side and then air dried for at least 3 hours in a horizontal position without allowing the blood to touch any surface during drying, including other parts of the card. (Example on the right)
Storage/Transport
Store the dried blood samples at room temperature in the envelopes provided by the MSPHL and transport within 24 hours of collection.
Acceptable Specimen Type(s)
Initial Screen (the red form) or Repeat Screen (the green form)
Test Request Form(s)
Included in kit
Possible Results
Normal - The final newborn screening reports are mailed to the submitter and physician of record.
Low Risk - Repeat the newborn screen. If, however, the infant is sick or displays signs of metabolic distress, the physician may wish to conduct diagnostic testing instead of, or in addition to the repeat screen. The final newborn screening reports are mailed to the submitter and physician of record.
Moderate/High Risk - Diagnostic testing and consultation with a metabolic specialist is needed. Final results are phoned and faxed to physician/health care provider and appropriate follow up center. Follow up centers are contracted by the Department of Health and Senior Services (DHSS) for follow up tracking, testing, diagnosis, and counseling.
Interfering Substances
The marker analytes usually spike to a certain degree immediately after birth in affected newborns. This can be especially noticeable in infants that are breast fed only due to the longer fast that is imposed until the mother’s milk production begins. As the infant feeds regularly for a few days, the marker analytes will lower in concentration, but usually continue to remain above the established cutoffs. Prematurity and illness can affect the newborn screening results.
NICU Guidelines and Key for NBS
The recommended collection time between 24 and 48 hours after birth is adequate. Waiting too many days after birth to collect a newborn screening sample could jeopardize the detection of some fatty acid disorders. It is recommended that samples for confirmatory testing of abnormal fatty acid disorder screens be drawn immediately before a feeding time.
Result Reported
1 to 3 working days after receipt of specimen
Fees
$130 charge - for full panel of screening disorders.
CPT Codes
83789
LOINC/SNOMED Codes
N/A
Additional Information
Prevalence of Disorder: 1:5,000 in Missouri
For more information on this Disorder, visit the DHSS Newborn Screening website.